
Abortion procedures are wrong because they intentionally and directly kill preborn human beings, but they are also risky to women — and even abortion industry insiders, insurance companies, universities, and abortion-friendly groups admit that later in gestation (at a point at which babies have a chance to survive when born prematurely), they’re so dangerous that they should never be committed in an outpatient facility.
In part two of this series on late-term abortion, Live Action News will document what the aforementioned groups have stated about this topic. Read part one here.
Key Takeaways:
- Abortion always intentionally kills a human being, and is never justified.
- Even the abortion industry, insurers, and others admit that late-term induction abortions are so dangerous to women that they should never be committed in freestanding abortion facilities.
- Abortion businesses and their insurers should be warned that committing late-term abortions in non-hospital settings put women at great risk, and could land the businesses/insurers in legal hot water for operating outside the known ‘standard of care.’
The Context:
Induction abortion is the most common procedure used very late in gestation. The preborn child is typically injected with a feticide (often digoxin or potassium chloride) — either into the amniotic fluid, the head, or the heart — to induce cardiac arrest and death. The woman’s cervix is dilated over a period of days and she eventually experiences labor, giving birth to a stillborn baby.
This procedure is typically used for preborn children at 25 weeks gestation and later — well past the time a preborn child can survive outside the womb with medical assistance.
What’s Happening:
Today, freestanding late-term abortion facilities are popping up nationwide, potentially placing the women’s lives in danger by committing late-term abortions “for any particular reason” — in facilities that may not be equipped to handle life threatening complications.
As part one of our series pointed out, even a well-known late-term abortionist (now retired) stated on one of his facility’s consent forms that abortions at 18 weeks or later are more dangerous for women than carrying their babies to term.
Later abortion businesses often leave women unmonitored while they labor in hotel rooms, where women sometimes deliver their babies into toilets.
Examples of freestanding late-term facilities include:
- C.A.R.E. Clinic – Commits abortions up to 35 weeks in Maryland. Founded by the late abortionist LeRoy Carhart, the clinic website admits it commits induction abortion, which “ends with the start of labor and delivery of a stillborn.”
- Partners in Abortion Care – Commits “induction abortions with IV sedation beyond 26 weeks (third trimester) of pregnancy”
- DuPont Clinic – Commits “three-day abortion procedure… called the DuPont Induction-Evacuation” between 25 and 32 weeks gestation
- Women’s Choice Health Care Clinic of Colorado – Completes later abortions (to 32 weeks) with induction.
- ParkMed New York City – Trains through the Ryan Residency abortion training program, commits inductions for “abortions that occur in the second trimester or beyond”
- Hope Clinic – Commits “all trimester” abortions in Chicago, Illinois
- OHSU, Center for Women’s Health – Commits abortions up to 34 weeks in in Portland, Oregon
- VAG Clinic (Valley Abortion Group) – Commits abortions through 34 weeks in New Mexico
According to the Guttmacher Institute, “9 states and DC states do not restrict abortion based on gestational duration.”
Nationally, more than 10,000 abortions occur at or after 21 weeks every year.
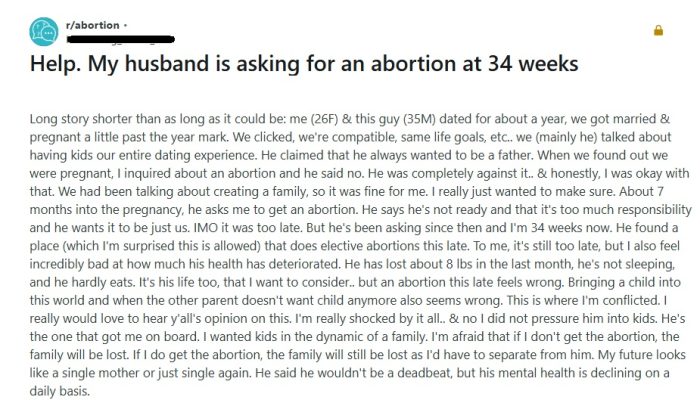
Reddit post on abortion at 34 weeks
Why It Matters:
To be clear: the intentional killing of a preborn child is unacceptable and is not health care — and that child still loses his or her life, whether in a hospital or an abortion facility.
In addition to the abortion industry’s grisly trade, women are being harmed — sometimes because proper medical protocols aren’t followed. And even though abortion isn’t true “care,” those necessary medical protocols are referred to here as the “standard of care.”
Medical malpractice attorney Mike Seibel told Straight Talk on Life Issues, “The standard of care is that they should be done in a hospital or hospital like setting… It’s very risky to do a late-term abortion… [E]ven [retired late-term abortionist] Curtis Boyd admits that it is very, very dangerous and it increases each week that you go on into the pregnancy.”
Abortion facilities committing these procedures outside a hospital setting, along with the insurance companies which cover the facilities, need to be warned that injuries to women (or even their deaths) could result in legal action with costly repercussions, Seibel said. When they are placed on notice, these freestanding abortion facilities may find it difficult to obtain or maintain malpractice insurance, because the standard of care indicates these completely unnecessary intentional killings should be committed in hospitals for women’s safety.
Insurers know the ‘standard of care’
Big Abortion places profit over the health of women — and those profits are hefty.
“Third trimester abortion costs can range from a couple thousand dollars to over $25,000, depending on how far along the pregnancy is and how clinically complex it is,” wrote pro-abortion KFF.org in 2024.
In 2016, Yahoo Parenting highlighted a woman who claimed that she paid $25,000 to “euthanize” a 36-week-old preborn baby via an induction abortion.
And yet, outpatient induction abortions are so dangerous to women that many insurance carriers will not cover them.
Even the guidance they offer online shows their awareness of the dangers:
- Presbyterian Health Plan, Inc. will cover “elective abortion,” but the group’s 2024 Group Subscriber Agreement and Guide to Your Managed Care Plan states that “Elective abortions after the 24th week of pregnancy are not covered.”
- Blue Cross/Blue Shield‘s January 1, 2025 medical policy, which uses The American College of Obstetricians and Gynecologists’ committee on coding and nomenclature on late-term abortions, states, “Labor-inducing abortions usually require hospitalization due to the possible risks to the mother if not closely monitored.”
- Cigna Insurance was clear in 2019 and 2021 that “Induction abortions must be done in a hospital so that you can be monitored during the entire procedure.” Today, Cigna’s website still indicates these late procedures should be conducted in hospitals, writing, “Induction abortion is ending a pregnancy by using medicines to start (induce) labor and delivery in the second or third trimester. This is done in the hospital.”
Cigna insurance – Induction abortions in hospitals
University hospitals know the ‘standard of care’
Various university hospitals also note that an induction abortion should be done “in the hospital”:
- University of Vermont Medical Center: “Induction abortion is ending a pregnancy by using medicines to start (induce) labor and delivery in the second or third trimester, This is done in the hospital.”
- Oregon Health and Science University’s (OHSU) Center for Women’s Health: “If you have a medication abortion to induce labor that ends a pregnancy, you will need to be in the hospital.”
- University of Rochester Medical Center (URMC):”Second-trimester medical abortions (or labor-induction terminations) are performed in the hospital.”
- New York-Presbyterian: “Induction abortion is ending a pregnancy by using medicines to start (induce) labor and delivery in the second or third trimester. This is done in the hospital. The doctor may also use a medicine to stop the pregnancy before induction.”
- Northshore Endeavor Health: NEH unites “nine top regional hospitals and connecting over 300 care locations across Chicagoland” and says “Induction abortion is ending a pregnancy by using medicines to start (induce) labor and delivery in the second or third trimester. This is done in the hospital.”
- Kaiser Permanente has similar language.
-
Kaiser Permanente – Induction abortions in hospitals
University of Vermont – Induction abortion in hospitals
Pro-abortion groups know the ‘standard of care’
The American College of Obstetricians and Gynecologists (ACOG)
ACOG appears to have slightly altered its stance over the years.
- 2006: ACOG claimed that later induction abortion procedures had to be committed in hospitals, writing in an amicus brief in the Gonzales v. Carhart case (emphasis added):
Other than D&E, almost all other induced abortions after the first trimester are performed by the method known as induction. In an induction abortion, the physician induces pre-term labor with potent medications, the cervix dilates, and the fetus is generally expelled through the labor process. The procedure requires constant monitoring and must be performed in a hospital.”
- 2011: ACOG’s FAQ on abortion stated, “Early surgical and medical abortions can be done safely in a health care provider’s office or clinic. Later abortions often are performed in hospitals or in special clinics.”
- 2015: ACOG’s FAQ read, “Second-trimester medical abortion usually is done in a hospital or clinic where you can be monitored throughout the procedure.”
- 2021: ACOG’s amicus brief in the case of Whole Woman’s Health v. Paxton, ACOG footnoted (emphasis added):
Although medical induction is generally safe, it does involve risks and side effects that D&E does not, such as a risk of uterine rupture, a rare but potentially life-threatening condition, and a retained placenta, a condition which can cause hemorrhaging and requires a surgical intervention… Because of the complications associated with labor, medical induction occurs in a hospital or hospital-like facility.
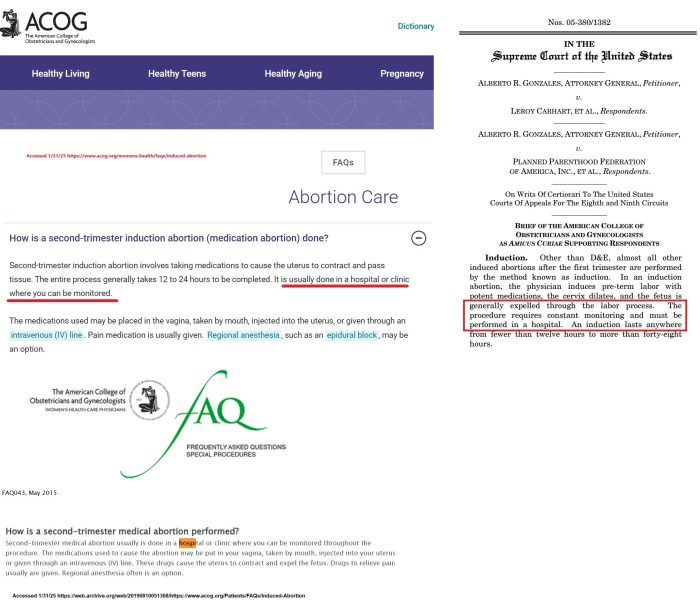
ACOG on induction abortion website (2011+2015) v amicus brief
Late-Term Abortion Initiative
Even when the abortion is induced medically (using abortion pills), the pro-abortion Late-Term Abortion Initiative acknowledges that “Medical induction most commonly occurs in hospitals on a labor and delivery unit or a family planning unit within the hospital.”
LTAI adds that “approximately 8% of women who undergo induction abortion require a surgical procedure for retained placenta.”
Guttmacher Institute
The Guttmacher Institute, a former “special affiliate” to Planned Parenthood, wrote in 2017, “… [T]ypically, induction takes longer than D&E, is more expensive, and is performed in a hospital setting” (emphasis added).
The footnote references a Dilation and Evacuation chapter in a book on abortion. as well as ACOG’s “Second-trimester abortion,” 2013 Practice Bulletin No. 135.
The Bottom Line:
Abortion-supporting organizations, university hospitals, and insurers all know that late induction abortions should be committed only in hospitals to mitigate the risks to women.
So, why are these gruesome procedures being done elsewhere, and will anything be done to stop them?
Follow Live Action News on Facebook and Instagram for more pro-life news.





