
Though there is never a reason to intentionally end the life of a preborn child by abortion, the abortion industry does so even while it knowingly puts women at risk — especially by violating the “standard of care” when it comes to late-term abortions.
As Live Action News has already shown, abortionists are aware that, at a certain point in the second trimester, abortion becomes far more risky to women than carrying to term. In addition, the industry knows that in doing late-term abortions outside hospital or hospital-like settings, it is violating the ‘standard of care’ and putting women at significantly greater risk. But knowing and doing are two different things… and an industry that intentionally and electively kills human beings clearly cannot be trusted to care about the safety of women or their children.
So why are taxpayer dollars being funneled to abortionists who not only kill children but put women at risk by violating the ‘standard of care’?
Key Takeaways:
- Abortionists and others know that committing induction abortions late in pregnancy outside hospital settings does not follow the ‘standard of care.’
- Multiple states fund these late-term abortions using their portion of Medicaid (state taxpayer) dollars, even though using federal Medicaid is not allowed because of the federal Hyde Amendment.
- In states where Medicaid is used to pay for abortions, 70% of those utilizing it for this reason were Black, and 66% were Latino, showing that taxpayers are largely paying for the deaths of minorities.
The Backstory:
In 2015, medical malpractice attorney Mike Seibel investigated a Ryan Residency abortion training program at the University of New Mexico (UNM), later winning a malpractice lawsuit against abortionist Curtis Boyd with co-counsel Justin Hall. Seibel discovered that 23 year-old Keisha Atkins had been given the abortion pill regimen during her 24-week induction abortion as part of an experiment at Boyd’s Southwestern Women’s Options (SWO) in Albuquerque, New Mexico. Atkins died as a result of the abortion.
Boyd has admitted to ending the lives of 250,ooo preborn babies.
Seibel told Live Action News that the abortion industry knows committing later abortions in outpatient facilities is more dangerous for woman, emphasizing that “The Standard of Care is that they should be done in a hospital or hospital-like setting” due to the risks involved.

Medical malpractice attorney Mike Seibel
Abortion industry experts have even testified in court that they are aware that the ‘standard of care’ for late-term induction abortions is that they take place within hospitals or hospital-like facilities.
“A doctor or clinic that performs an induction abortion outside of a hospital or hospital-like facility would expose a patient to needless danger,” claimed Seibel. “We have a whole bunch of testimony from the abortion industry itself saying ‘this is below the standard of care,'” Seibel said, “and, because they are violating the standard of care, they should not be eligible for Medicaid reimbursements.”
The Details:
Is Medicaid funding late-term induction abortions that do not conform to the ‘standard of care’?
Medicaid can be used to fund late-term abortions, despite federal Hyde Amendment prohibitions, which “ban[] state use of federal Medicaid dollars to pay for abortions unless the pregnancy is the result of rape or incest, or the abortion is ‘necessary to save the life of the woman.'” States, however, decide whether or not to use their portion of those dollars to pay for the killing of preborn babies — at any stage of development, for any reason.
According to a May 2025 report from the pro-abortion Guttmacher Institute, “9 states [Alaska, Colorado, Maryland, Michigan, Minnesota, New Jersey, New Mexico, Oregon, and Vermont] and the District of Columbia do not restrict abortion on the basis of gestational duration.”
The U.S. Supreme Court ruled that taxpayer-funding of abortions could be limited. Despite the Hyde Amendment, taxpayer dollars still fund some abortions for any reason at the state level, according to expenditure reports at Medicaid.gov.
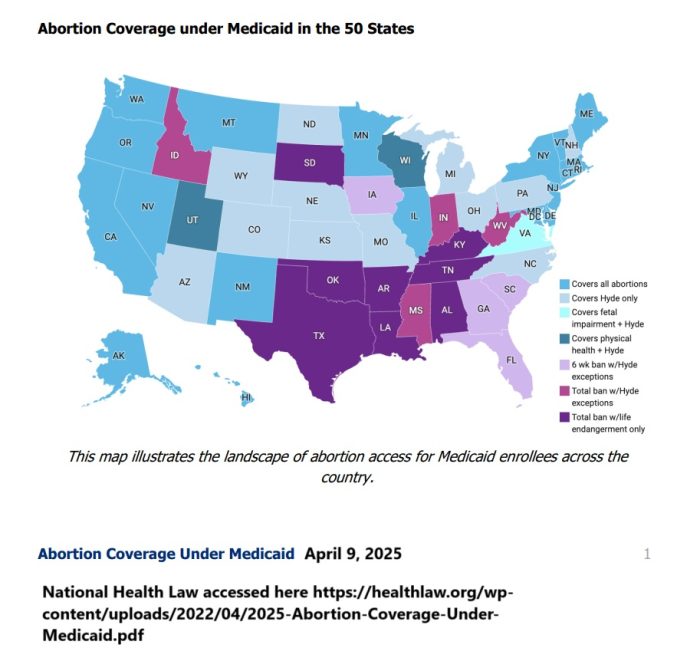
Abortion Coverage under Medicaid National Health Law April 2025
Which state Medicaid programs pay for abortion, regardless of gestational age?
As of March 12, 2025, the pro-abortion Guttmacher Institute claimed that “19 states [Alaska, California, Connecticut, Delaware, Hawaii, Illinois, Maine, Maryland, Massachusetts, Minnesota, Montana, Nevada, New Jersey, New Mexico, New York, Oregon, Rhode Island, Vermont, and Washington] have a policy or court order that directs state Medicaid funds to pay for abortions under all circumstances….”
The pro-abortion Kaiser Family Foundation (KFF) reported that 20 states fund abortions, “exceeding federal requirements,” adding Colorado in addition to the 19 listed by Guttmacher.
Only “7 states [Alaska, Kentucky, New York, North Carolina, Oklahoma, South Dakota, and West Virginia] require providers to indicate the method of payment,” Guttmacher claimed.
In some states that pay for abortions, there are no limits for reasons or gestational age. Here are some examples:
- California – “Abortion is a covered benefit regardless of the gestational age of the fetus” (emphasis added) and “Medical justification and authorization for abortion are not required,” the state’s Medi-Cal program stated in 2024. Between 2014 and 2020, California taxpayers funded approximately 411,000 abortions, costing nearly $118M, according to data from the State’s Medi-Cal website. But between 1989 to 2020, the state’s taxpayer-funded abortions had reached nearly one billion dollars ($785,421,873).
- Colorado – A fiscal analysis, in the state where late term abortionist Warren Hern previously operated, literally claimed that taxpayer-funded abortion (projected at nearly $5.9 million in FY2026-27 ) would save taxpayers money because it would prevent births.
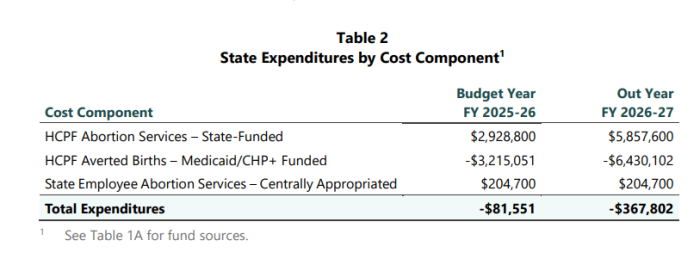
Colorado abortion v Medicaid averted births
- Maryland – The most current data on state taxpayer dollars funding abortion (which may not include all abortions), shows that in 2006, the state funded 3,831 abortions at a price tag of $2.7M. Just 10 years later, in 2016, that number had more than doubled to 7,897 abortions at double the cost — $5.4M. By 2020, just four years later, the state paid for 9,864 abortions at a cost of $6.5M.
2020: $6.5 million /9,864 abortions
2019: $$6.1 million/9,676 abortions
2018: $6.3 million /9,875 abortions
2017: $5.7 million / 8,798 abortions
2016: $5.4 million / 7,897 abortions
2015: $5.7 million / 7,945 abortions
2014: $5.6 million / 7,651 abortions
2013: $5.4 million / 7,528 abortions
2012: $5.2 million / 7,442 abortions
2011: $5.4 million / 7,177 abortions
2010: $4.7 million / 6,652 abortions
2009: $3.4 million / 4,857 abortions
2008: $2.2 million / 3,281 abortions
2007: $2.2 million / 3,580 abortions
2006: $2.7 million / 3,831 abortions
- Minnesota – “There is no law limiting the availability of abortion based on how far along in pregnancy you are,” claimed one online abortion locator. Minnesota’s Attorney General website is clear that “Minnesota law no longer requires that abortions be performed in a hospital, and facilities like birthing centers can now offer abortions.” The site also states that “qualifying patients” can receive “public assistance… to cover or partially cover the cost of reproductive health care services, including abortion,” and that those qualifying for Medicaid and Minnesota Care may also be able to receive taxpayer funded abortions, adding, ‘The use of these funds is no longer limited to instances of rape or incest, or where the pregnant person’s health is in danger.” A state evaluation claimed that “10,166 Minnesota residents had an induced abortion in 2022. Of these abortions, 48% were covered by state public insurance, 33.5% were self-pay, and 18.5% were covered by commercial plans.”
- New Mexico – “Abortion is not restricted based on gestational duration” and “State Medicaid funds cover abortion,” claimed Guttmacher. (The same was true for Alaska (previously documented by Live Action News), Maryland, New Jersey, Oregon, and Vermont.) In just two years (2020 and 2021), New Mexico spent nearly $1 million tax dollars funding 7,327 abortions,” Abortion Free New Mexico (AFNM) reported. Previous data “reveals from 2017-2019 state taxpayers paid $791,106.50 for 5,889 abortions,” AFNM wrote.
- New York – Abortions are taxpayer-funded and available into the third trimester of pregnancy. State data reveals that 34,054 (nearly half) of the 68,388 total abortions committed in 2022 were funded by Medicaid, nearly 50% in 2021, and nearly 49% in 2020. Live Action News previously documented a breakdown of induced abortion from the New York Department of Health, which revealed 44% of the total abortions committed in 2012 were tax funded, nearly 46% in 2013, 47% in 2014, 49% in 2015.
- Oregon – According to the Oregonian, abortions are covered under the Oregon Health Plan, “which paid $2.4 million for 3,769 abortions in 2016, according to Oregon Health Authority documents.”
- Washington State – WA’s Medicaid, Apple Health, lists “Apple Health Pregnancy Related Services” in its Medicaid guide for 2025. It states that covered services include “voluntary terminations,” including “spontaneous, incomplete, missed, induced, and elective abortions….” The carrier “pays for surgical abortions that occur in an ambulatory surgical center (ASC), hospital…. Abortion centers must be approved by and contracted with HCA to bill for facility fee payments for a surgical abortion…. Abortion centers are reimbursed the facility fees only for surgical abortions.”
Reality Check:
When “low-income” translates primarily to communities of color
Abortion is tethered to eugenics — so it is no surprise that studies have shown that in some states, Medicaid-funded abortions appear higher among targeted communities of color.
The Guttmacher Institute analyzed state-funded abortion, and noted in February of 2024 that “Medicaid usage for abortion care was highest among respondents in Medicaid states who identified as Black (70%), Latinx (66%), had one or more prior births (70%–77%), those having second-trimester abortions (75%) and those with the lowest incomes (78%). ”
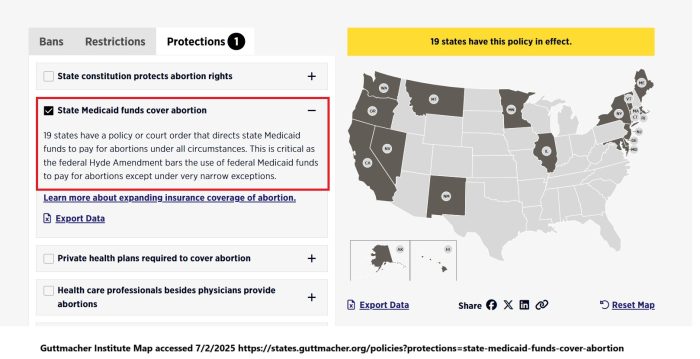
Guttmacher Institute 19 states fund abortion via state Medicaid dollars
Live Action News previously documented how funding abortion — as well as ease of access and location to abortion facility, plays a role in increased abortions. This is a win for abortion profiteers.
A 2024 study found that “In Maine and Illinois, implementing state Medicaid coverage of abortion contributed to an immediate overall increase in abortion access….” Another found that “Between 2017 and 2020, Illinois and Maine introduced Medicaid funding of abortion and the abortion rate increased by 14 and four abortions per 1000 Medicaid insured women, respectively.”
“When Illinois introduced Medicaid coverage for abortion, the abortion rate increased by 2.4 per 1,000 women (18.2%) and births decreased by 1.7 per 1,000 women (2.8%). Decreases in birth rates were higher among Black and Hispanic people, people in low-income areas, and for people who lived closer to an abortion facility,” reported the University of Maryland School of Public Health.

A separate study concluded that “Medicaid coverage of abortion care is associated with a much higher lifetime incidence of abortion among individuals insured by Medicaid. We infer that Medicaid coverage of abortion care costs may have a very large impact on the accessibility of abortion care for low‐income women.”
“We find evidence that in Maryland, a state that has long provided Medicaid funding for low-income women’s abortion care, women insured by Medicaid are much more likely to have had an abortion over their reproductive lifetimes than are Maryland residents not insured by Medicaid,” authors wrote.
Taxpayers shouldn’t be paying for this
According to the Kaiser Family Foundation (KFF.org), “There is tremendous variability in how much states reimburse for abortion services in states that use state funds to pay for abortions under Medicaid”:
- Medication abortion: $162 (RI) to $665 (NM)
- D&C procedures: $146 (WA) to $1,000 (NY)
- D&E procedures: $248 (WA) to $1,300 (NY), $1,920 (IL)
“In recent years, some states, such as Illinois, New York, New Mexico, and Maryland have significantly boosted their Medicaid reimbursement rates to support abortion access in their states in the face of abortion bans and restrictions in states across the nation. For example, six states have more than doubled their reimbursement rates for D&C procedures and five states for D&E procedures since 2017,” KFF.org wrote (emphasis added).
“In states that fund abortion services for Medicaid enrollees the median reimbursement for a D&E procedure was $570, ranging from a low of $248 in Rhode Island and Washington to a high of $1,920 in Illinois,” KFF added.
Induction abortions, which are generally committed at 25 weeks gestation and later — and should only be committed in a hospital, according to some abortion providers — cost far more.
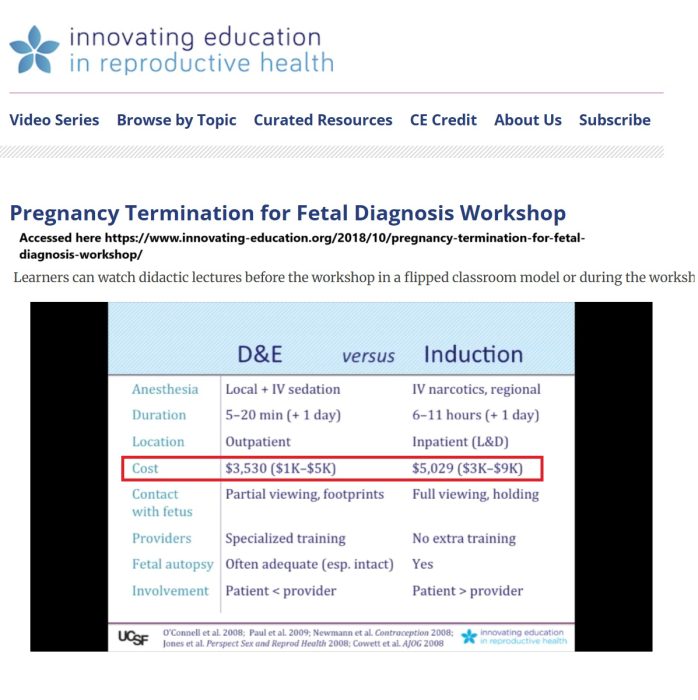
Cost of late term abortions (Innovating Education)
“Third trimester abortion costs can range from a couple thousand dollars to over $25,000, depending on how far along the pregnancy is and how clinically complex it is,” wrote KFF.
In 2016, Yahoo Parenting highlighted a woman who claimed that she paid $25,000 to “euthanize” her 36-week-old preborn baby via induction abortion.
A recent decision from the U.S. Supreme Court in the case of Medina v. Planned Parenthood South Atlantic will allow states to redirect taxpayer dollars away from abortion facilities; perhaps more states should enact these measures.
Live Action News will detail putting the late term abortion industry on notice for violating the ‘standard of care’ in the next article of this series.
Follow Live Action News on Facebook and Instagram for more pro-life news.





